Research
Campus Maps
Understanding Cognitive Deficits in Parkinson’s Disease and Striatum-mediated Cognition
About Penny MacDonald

Dr. Penny MacDonald is a Movement Disorders Neurologist and Assistant Professor in the Department of Clinical Neurological Sciences, and a Principal Investigator at the Brain and Mind Institute. She is cross-appointed in the Departments of Neuroscience, Physiology and Pharmacology, and Psychology.
Background to the Research
Parkinson’s disease (PD) is a common movement disorder characterized by motor symptoms of tremor, stiffness, and slowness, affecting 1-2% of Canadians over the age of 65. Dr. MacDonald’s research aims to understand the nature and causes of cognitive deficits such as learning, memory, and thinking problems that are increasingly recognized in more than 50% of PD patients. Deficits in cognition disproportionately cause a decline in quality of life for patients with PD, and are a frequent cause of institutionalization. Clarifying these deficits and the changes in brain function that underlie them is therefore critical.
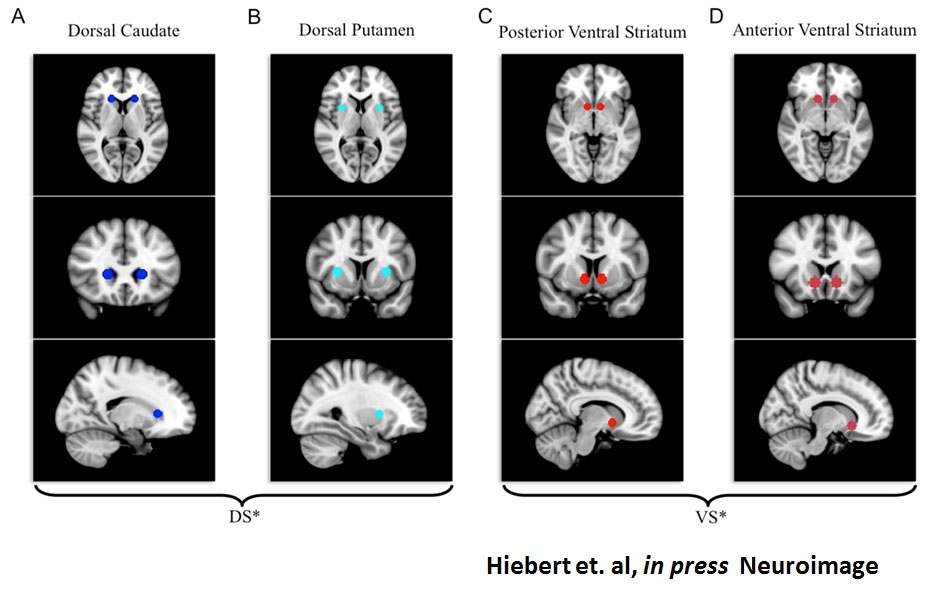
Toward understanding cognitive problems in PD, Dr. MacDonald’s research also aims to clarify cognitive functions performed by the striatum, a subcortical brain region implicated in movement initiation and regulation, as well as increasingly in cognition. In PD, neurons producing dopamine degenerate at a faster than normal rate. Dopamine is an important chemical messenger in the brain. The dorsal part of the striatum is especially dopamine depleted in PD and this dopamine deficit is the cause for the movement symptoms and some cognitive deficits in PD. The ventral part of the striatum and other brain regions such as the frontal and limbic cortices receive closer-to-normal dopamine supply especially at early stages of PD. This understanding allows us to predict which functions will improve versus worsen due to the dopamine-replacement medications that are prescribed to improve movement symptoms. In this way, identifying cognitive functions performed by the dorsal and ventral parts of striatum will at least partially explain the cognitive profile in PD and how cognitive functions respond to dopaminergic medication.
Research Approach

Dr. MacDonald tests PD patients ON and OFF dopaminergic therapy compared to age-matched, healthy control participants on a host of cognitive and behavioural tests to better define the cognitive profile in PD. She also uses functional magnetic resonance imaging (fMRI) to measure changes in regional brain activity associated with cognitive functions, relating these observations to cognition in PD.
Results
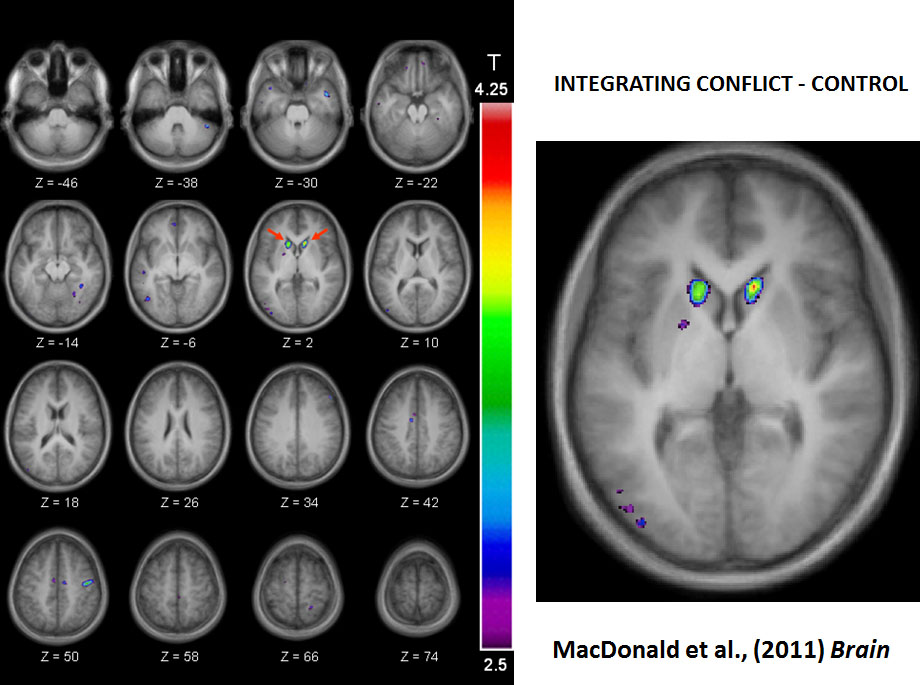
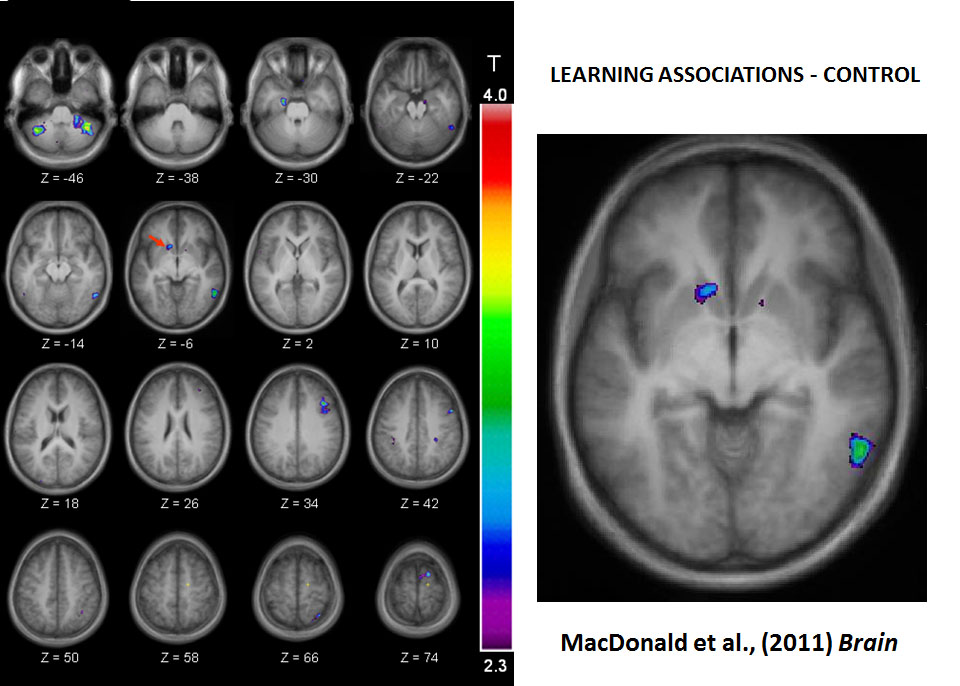
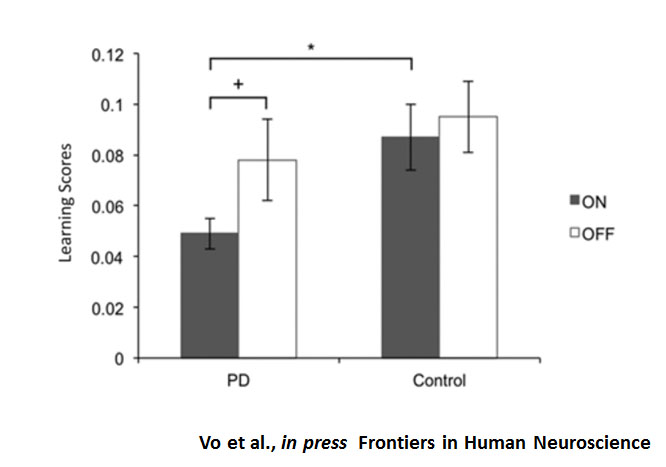 To this point, Dr. MacDonald has found that decision-making or selecting responses, especially when this requires reconciling conflicting information, is impaired in PD patients but improves when treated with dopaminergic therapy 1, 2. In contrast, PD patients learn associations between stimuli, responses, or rewards as well as age-matched healthy controls when they are tested off dopamine-replacement therapy. Dopamine-replacement therapy worsens association and list learning, especially at early stages of disease 3-6.
To this point, Dr. MacDonald has found that decision-making or selecting responses, especially when this requires reconciling conflicting information, is impaired in PD patients but improves when treated with dopaminergic therapy 1, 2. In contrast, PD patients learn associations between stimuli, responses, or rewards as well as age-matched healthy controls when they are tested off dopamine-replacement therapy. Dopamine-replacement therapy worsens association and list learning, especially at early stages of disease 3-6.
Making sense of these patterns in PD, using fMRI in healthy young volunteers, Dr. MacDonald has shown that dorsal parts of striatum underlie decision making and selecting specific responses, whereas ventral parts of striatum are preferentially active at the time of learning associations 1, 7.
Future directions
PD is not the only disease that implicates the striatum. Dr. MacDonald is extending her research on the striatum to better explain cognitive problems in other conditions, such as Obsessive Compulsive Disorder and substance abuse, that are associated with striatal dysfunction.
References
1. MacDonald PA, MacDonald AA, Seergobin KN, Tamjeedi R, Ganjavi H, Provost JS, et al. The effect of dopamine therapy on ventral and dorsal striatum-mediated cognition in Parkinson's disease: support from functional MRI. Brain : a journal of neurology. 2011; 134(Pt 5): 1447-63.
2. MacDonald AA, Seergobin KN, Tamjeedi R, Owen AM, Provost JS, Monchi O, et al. Examining dorsal striatum in cognitive effort using Parkinson's disease and fMRI. Annals of Clinical and Translational Neurology. 2014; 1(6): 390-400.
3. MacDonald AA, Monchi O, Seergobin KN, Ganjavi H, Tamjeedi R, MacDonald PA. Parkinson's disease duration determines effect of dopaminergic therapy on ventral striatum function. Movement disorders : official journal of the Movement Disorder Society. 2013; 28(2): 153-60.
4. MacDonald AA, Seergobin KN, Owen AM, Tamjeedi R, Monchi O, Ganjavi H, et al. Differential effects of Parkinson's disease and dopamine replacement on memory encoding and retrieval. PloS one. 2013; 8(9): e74044.
5. Vo A, Hiebert NM, Seergobin KN, Solcz S, Partridge A, MacDonald PA. Dopaminergic medication impairs learning but not decision making in Parkinson’s disease. Frontiers of Human Neuroscience. 2014; (in press).
6. Hiebert NM, Seergobin KN, Vo A, Ganjavi H, MacDonald PA. Dopaminergic therapy affects learning and impulsivity in Parkinson’s disease. Annals of Clinical and Translational Neurology. 2014; (in press).
7. Hiebert NM, Vo A, Hampshire A, Owen AM, Seergobin KN, MacDonald PA. Striatum in stimulus-response learning via feedback and in decision making. NeuroImage. 2014; 101C: 448-57.