Current Areas of Interest
Studies and Ongoing Research Interests
Effectiveness of a novel Speech-in-Noise Treatment program for Hypophonia in Parkinson’s disease
Effectiveness of a novel Speech-in-Noise Treatment program for Hypophonia in Parkinson’s disease
Brief Description:
The Speech-in-Noise (SIN) treatment program was developed by Professor Scott Adams for the treatment of hypophonia in individuals with Parkinson’s disease (IWPD). It involves training higher speech intensity levels and speech-to-noise levels during variable levels (60-75dB SPL) of different types of background noise (multi-talker noise, traffic noise, white noise, etc.) while receiving real-time intensity feedback from a speech therapist in social situations inside and outside of the clinic. The SIN treatment program involves twelve, one-hour, speech therapy sessions over a 4-week period (3 sessions per week) combined with twelve, one-hour home-practice sessions (3 times per week).
Figure 1. Participant and SLP student during SIN treatment session.
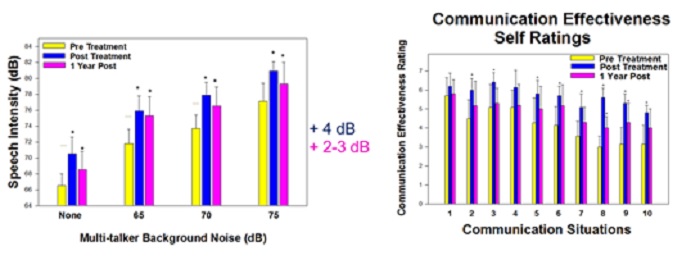
Figure 2. SIN & improved speech intensity. Figure 3. SIN & improved communication
effectiveness.
Results:
A pilot study investigating the effectiveness of the SIN treatment program in 7 individuals with Parkinson’s disease (IWPD) was completed and presented at a recent motor speech conference1. Following the SIN treatment program, the 7 IWPD demonstrated increased speech intensity (+4 dB) and SNR levels (+5 dB) for assessments obtained in the speech clinic but objective acoustic measures related to the transfer of treatment were not obtained. Results from two questionnaires suggest that transfer of treatment may have occurred but objective, out-of-clinic, speech intensity measures are required to confirm this effect. A grant from the Weston Brain Institute was recently received and will be used to conduct a larger clinical trial on the effectiveness of the Speech-in-Noise treatment program.
Link to clinical trial: https://www.clinicaltrials.gov/ct2/show/NCT04323085?term=NCT04323085&draw=2&rank=1
Use of a new portable Speech-to-Noise Feedback device for conversational hypophonia in Parkinson’s disease
Use of a new portable Speech-to-Noise Feedback device for conversational hypophonia in Parkinson’s disease
Brief Description:
The Speech-to-Noise Feedback (SNF) Device, and the related treatment program, involve a wearable device (developed by Scott Adams & Vijay Parsa) that provides continuous feedback about the participant’s conversational speech intensity level in most social situations outside of the clinic. The SNF device treatment program involves twelve, one-hour device experience and practice sessions over a 4-week period. These sessions involve conversations with a clinician in various background noise conditions in the clinic while wearing and receiving feedback from the SNF device. During the 4-week period, participants also wear the SNF device during their daily social activities for twelve, one-hour periods (3 times per week). The SNF device collects and stores long-term data related to continuous speech-to-noise levels for use as a primary treatment outcome measure.
Additional details related to the SNF device program: The SNF device is based on a wearable Raspberry Pi system with audio inputs from a throat accelerometer and binaural head microphones, and audio feedback output (warning tone) to an earpiece. Note: the SNF device is currently undergoing refinements to improve its efficiency, durability, and ease of use.
Figure 1. New Speech-to-Noise Feedback (SNF) device.
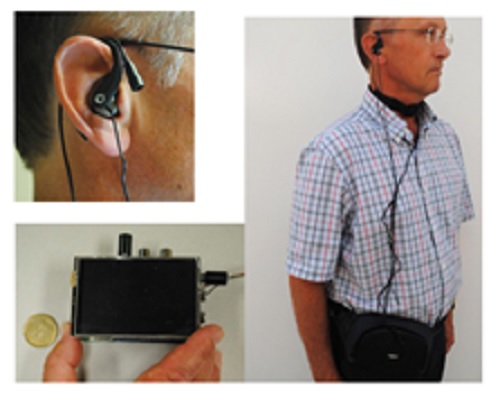
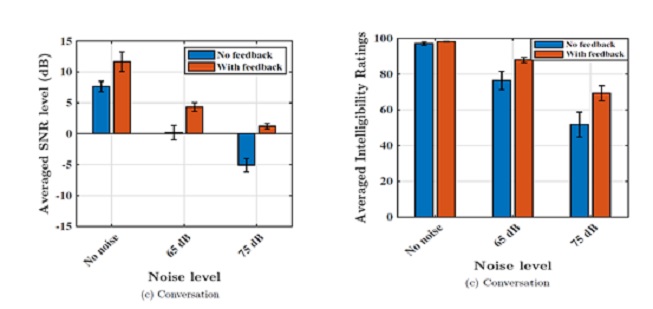
Figure 2. Preliminary results from 3 participants using the Speech-to-Noise Feedback (SNF) device during conversations in multi-talker noise conditions (none, 65db and 75dB). Average speech-to-noise ratio (SNR) level and average speech intelligibility rating scores are presented for the no feedback (SNF device-OFF) and with feedback (SNF device-ON) conditions.
Results:
A pilot study related to the new SNF device with 10 individuals using the device in the clinic for 2 hours was completed in 2019. Recently, a grant from the Weston Brain Institute was received to support a large clinical trial to study the effects of the SNF device treatment program on everyday conversational speech in a group of individuals with hypophonia related to Parkinson’s disease.
Link to clinical trial: https://www.clinicaltrials.gov/ct2/show/NCT04323085?term=NCT04323085&draw=2&rank=1
Comparison of Speech Amplifiers and Personal Communication Devices in Parkinson’s disease
Comparison of Speech Amplifiers and Personal Communication Devices in Parkinson’s disease
Brief Description:
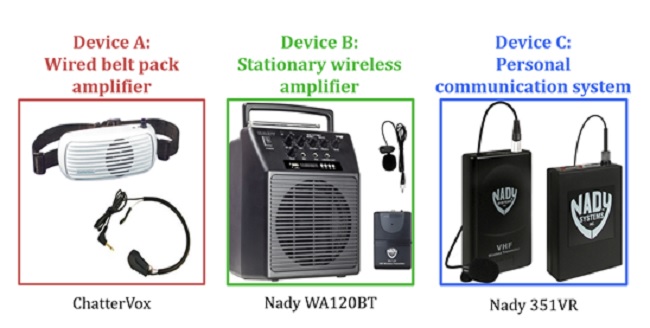
These research studies involve comparing the effectiveness and acceptance of different amplification devices in individuals with hypophonia related to Parkinson’s disease. Recent focus has been on the comparison of three types of amplification systems: a wired portable amplifier (Device A), a wireless stationary amplifier (Device B), and a one-way personal communication system (Device C). Outcome measures include speech-to-noise ratio, speech intelligibility, communication effectiveness ratings, and device acceptance.
Figure1. Examples of three amplification systems: a wired portable amplifier (Device A), a wireless stationary amplifier (Device B), and a one-way personal communication system (Device C).
Results:
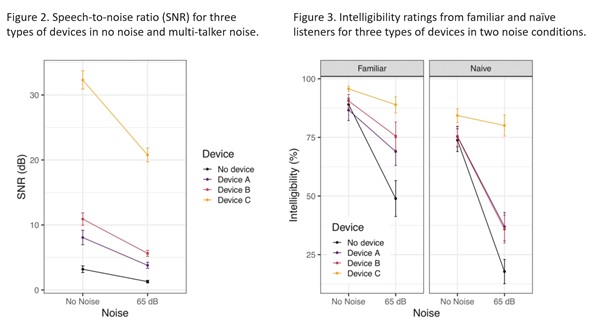
Results from a recent study of 22 individuals with Parkinson’s disease (Knowles et al., 2020) demonstrated clear differences in device performance in three distinct forms of amplification devices for individuals with HP. Findings suggest that amplification device use may be beneficial for this clinical population and underscore the potential to improve device availability and device selection criteria in future research.
This research continues in the SMD lab and in the recently developed Speech Amplifier Clinic in the Speech and Hearing Clinic in Elborn College at Western University.
Knowles et al. (2020): docs/articles/58 Knowles et al 2020 A comparison of speech amplification and personal communication devices for hypophonia.pdf
Andreetta et al. (2016): docs/articles/45 Andreetta et al 2016 Evaluation of speech amplification devices in Parkinsons disease.pdf
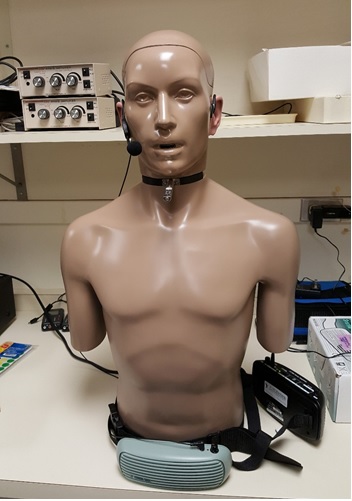
Figure 4. A head-torso simulator with mouth speaker (KEMAR) wearing a speech amplifier system (Chattervox).
Additional ongoing studies involve lab-based evaluations of the performance characteristics and listener preference ratings for different amplification systems.
Studies of self-loudness perception in Parkinson’s disease
Studies of self-loudness perception in Parkinson’s disease
Brief description:
These studies examine loudness perception in individuals with hypophonia and Parkinson’s disease. Loudness perception tasks include 1) magnitude estimation procedures involving a sentences spoken by another talker at different intensities (i.e. 60, 65, 70, 75 and 80 dB SPL), 2) imitation tasks involving a sentence spoken at different intensities, and 3) magnitude production procedures involving the self-production of sentences at different loudness levels (i.e. habitual, two and four times louder and two and four times quieter).
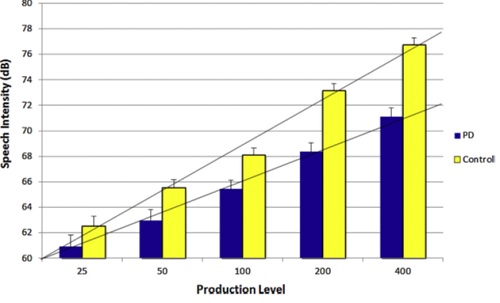
Figure 1. Average speech intensity produced by the PD and control participants for the 5 intended loudness levels (100= habitual, 200= two times louder, 400= four times louder, 50= two times quieter, and 25= four times quieter) during the magnitude production task.
Results:
The participants with PD were found to produce significantly different patterns and used a more restricted range than the controls in their perception of external speech loudness, imitation of speech intensity, and self-generated estimates of speech loudness. The results support a speech loudness perception deficit in PD involving an abnormal perception of externally generated and self-generated speech intensity.
Future studies will examine 1) the suppression of loudness perception during self-speech and 2) intensity control and self-loudness perception during self-amplified speech in individuals with hypophonia and Parkinson’s disease.
Clark et al. (2014): docs/articles/41 Clark et al 2014 Loudness perception and speech intensity control in Parkinsons disease.pdf
Altered auditory feedback effects on speech in Parkinson’s disease
Altered auditory feedback effects on speech in Parkinson’s disease
a) Altered intensity feedback
Brief description:
In these studies, the intensity of auditory feedback is systematically manipulated (i.e. increased or decreased by 5,10, and 15dB) during speech production and the resulting compensation in speech intensity is examined in individuals with Parkinson’s disease.
Figure 1. Setup for the altered intensity feedback experiments.
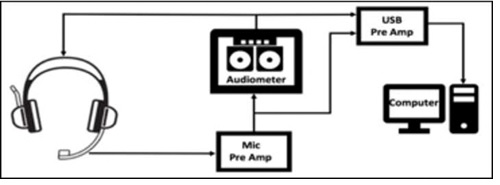
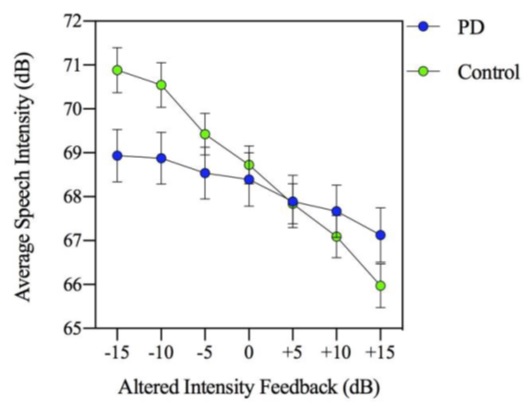
Figure 2. Average speech intensity during the 7 altered intensity feedback conditions.
Results:
Individuals with Parkinson’s disease displayed a reduced response to the altered intensity feedback compared to control participants. These results suggest that individuals with PD have abnormal processing of auditory information for speech intensity regulation.
Senthinathan (Abeyesekera), A., Adams, S., Page, A., & Jog, M. (2021). Speech intensity response to altered intensity feedback in individuals with Parkinson’s disease. Journal of Speech, Language, and Hearing Research, 64, 2261-2275. docs/Senthinathan-2021_JSLHR-20-00278.pdf
b) Multi-talker Masking noise and the Lombard effect on speech intensity
Brief description:
This study examined the effectiveness, satisfaction, and acceptance of a low-cost Lombard-response (LR) device in a group of individuals with Parkinson’s disease (IWPD) and their communication partners (CPs). Sixteen IWPD and hypophonia and their CPs participated in the study. The IWPD wore a LR device that included a small MP3 player (Sony Walkman) and headphones playing a multi-talker noise audio file at 80 dB during lab-based speech tasks and during their daily conversational speech over a 2-week device trial period. Outcome measures included average conversational speech intensity and scores on a questionnaire related to speech impairment, communication effectiveness, and device satisfaction.
Figure 1. Lombard-response device that includes an MP3 player and headphones playing multi-talker masking noise at 80-90dB SPL.
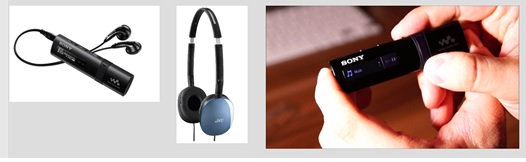
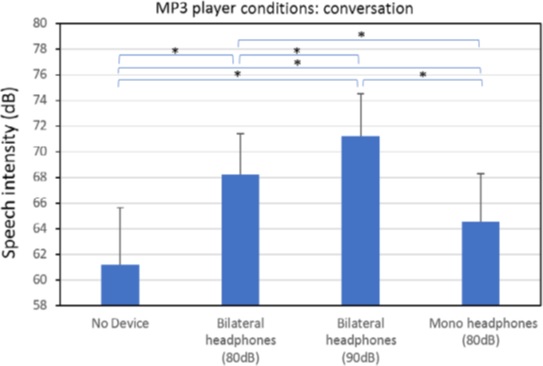
Figure 2: Average conversational speech intensity obtained from individuals with Parkinson’s disease during several Lombard-response device conditions.
Results:
Conversational speech intensity of the IWPD is increased by 7 to 10 dB with the LR device. Short-term acceptance and satisfaction with the LR device were moderate, but long-term acceptance, beyond 4 months, was absent. Future studies are required to determine if other types of low-cost LR devices can be developed that improve long-term efficacy and device acceptance in IWPD and hypophonia.
Adams et al. (2020): docs/articles/57 Adams et al 2020 Efficacy and acceptance of a Lombard-response device for hypophonia in Parkinsons disease.pdf
Effects of medications and surgical procedures on speech in Parkinson’s disease
Effects of medications and surgical procedures on speech in Parkinson’s disease
- a) Effects of levodopa (anti-parkinson) medication on speech in Parkinson’s
Brief description:
The effect of levodopa (anti-parkinson) medication on measures of voice quality was examined in fifty-one individuals with Parkinson’s disease (IWPD). IWPDs produced prolonged vowels while on and off levodopa and a perceptual measure of overall voice quality was obtained from 3 listeners.
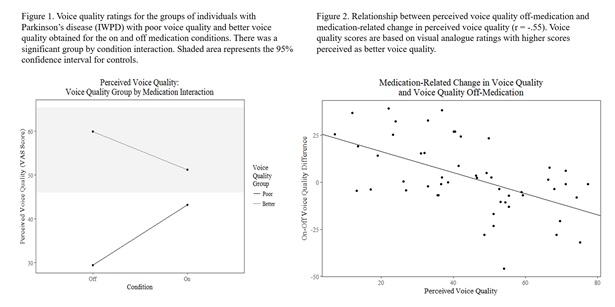
Results:
When the IWPDs were examined as a group, no significant difference was found between on and off levodopa conditions. In contrast, when IWPDs were split into two groups based on voice quality severity, a significant group-by-medication state interaction emerged. In addition, there was a significant correlation (r=.55) between the magnitude of levodopa-related improvement in perceived voice quality and voice quality severity. Results do not support the hypothesis of reduced levodopa- responsiveness to voice symptoms as disease duration increases. Instead, the results suggest that the magnitude of the levodopa response may increase with increasing severity of the voice quality symptoms. These results suggest that the severity of speech and voice symptoms needs to be given greater consideration in future studies of levodopa effectiveness in individuals with Parkinson’s disease.
Additional studies in our lab have found a similar relationship between increasing speech symptom severity and increased responsiveness to levodopa medication for speech intensity and speech dysfluency in individuals with Parkinson’s. Ongoing studies are examining the levodopa effects on speech intelligibility, consonant acoustics and rate of speech.
Cushnie-Sparrow et al. (2018): docs/articles/48 Cushnie-Sparrow et al 2018 Voice quality severity and response to levodopa in Parkinsons disease.pdf
Im et al. (2019): docs/articles/54 Im et al 2019 Effect of levodopa on speech dysfluency in PD.pdf
Pieterman et al. (2018): docs/articles/49 Pieterman Adams Jog 2018 Method of Levodopa Response Calculation Determines Strength of Association with Clinical Factors in Parkinson Disease.pdf
b) Effects of Deep Brain Stimulation on speech in Parkinson’s
Brief description:
The purpose of these studies is to systematically evaluate the effect of deep brain stimulation of the subthalamic nucleus (STN-DBS) on speech in Parkinson's disease. Systematic changes in the amplitude, frequency, and pulse-width electrical parameter settings were examined over multiple sessions. The effects of these different stimulation settings were examined for speech intelligibility, vowel acoustic space, speech intensity, speech prosody and voice quality.
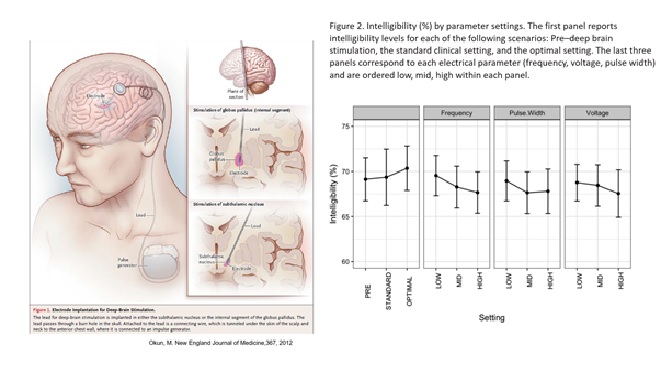
Results:
Overall, a lower-frequency STN-DBS stimulation (60 Hz) was found to lead to improvements in intelligibility and acoustic vowel expansion. In addition, the combinations of lower frequency, lower pulse width, and higher voltage settings were associated with improved speech intensity, voice quality and speech prosody. These studies indicate that standard clinical DBS settings may not be optimized for speech symptom improvements and that alternate settings, particularly lower stimulation frequencies could be used as a starting point for improving speech outcomes in DBS treatment for Parkinson's disease.
Knowles et al. (2017): docs/articles/47 Knowles et al 2017 Deep brain stimulation parameter optimization for vowel acoustics and speech intelligibility in Parkinsons disease.pdf
Abeyesekera et al. (2019): docs/articles/52 Abeyesekera et al 2019 Effects of_deep brain stimulation of the subthalamic nucleus settings on voice quality intensity and prosody in parkinsons disease preliminary evidence for speech optimization.pdf
Concurrent manual and gait tasks on speech intensity
Concurrent manual and gait tasks on speech intensity
Brief description:
These studies focus on the effect of a concurrent task on speech intensity in individuals with Parkinson’s disease. One concurrent task was a visuomotor manual tracking task that involved squeezing a hand bulb that generated a continuous signal that was used to track a moving target (0.2Hz sinusoid) on a computer screen. A second concurrent task examined the effect of concurrent walking tasks (slow, normal, fast) on conversational speech intensity.
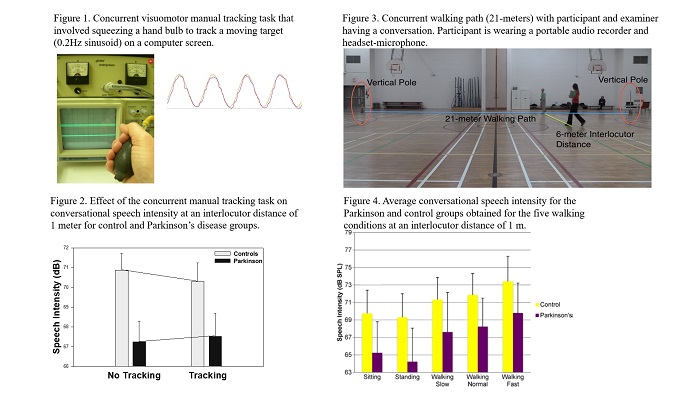
Results:
The concurrent manual tracking task was associated with a significant and consistent reduction in speech intensity for the control participants but a significant increase or enhancing effect on conversational speech intensity in the participants with PD. For the concurrent walking task, concurrent walking was found to produce a significant increase in speech intensity, relative to standing and sitting, in both the control and PD groups. In addition, faster walking produced significantly greater speech intensity than slower walking.
The results of these studies indicate that concurrent manual and walking tasks can have an energizing effect on conversational speech intensity in persons with hypophonia and Parkinson’s disease. These positive, ‘‘energizing’’ effects need to be given consideration in future attempts to develop a comprehensive model of speech intensity regulation and they may have important implications for the development of new evaluation and treatment procedures for individuals with hypophonia related to PD.
McCaig et al. (2016): docs/articles/44 McCaig et al 2016 Effect of concurrent walking and interlocutor distance on conversational speech intensity and rate in Parkinsons disease.pdf
Adams et al. (2010): docs/articles/37 Adams et al 2010 Effects of Interlocutor Distance, Multi-talker Background Noise, and a Concurrent Manual Task on Speech Intensity in Parkinsons Disease.pdf
New measures of speech loudness and hypophonia severity
New measures of speech loudness and hypophonia severity
1. Modelling loudness: Acoustic and perceptual correlates in the context of hypophonia in Parkinson’s disease
Daryn Cushnie-Sparrow's PhD thesis (2021): docs/Daryn-Cushnie_Sparrow-PhD-2021-Acoustic-and-perceptual-correlates-of-loudness-in-Parkinson_s-disease.pdf
Abstract
Hypophonia (quiet speech) is a common speech symptom associated with
Parkinson’s disease (PD), and is associated with reduced intelligibility,
communicative effectiveness, and communicative participation. Studies of
hypophonia commonly employ average speech intensity as the primary dependent
measure, which may not entirely capture loudness deficits. Loudness may also be
affected by the frequency components of speech (i.e. spectral balance) and speech
level variability. The present investigation examined relationships between
perceived loudness and intelligibility with acoustic measures of loudness, speech
intensity, and spectral distribution in individuals with hypophonia secondary to
Parkinson’s disease (IWPDs) and neurologically healthy older adults (HOAs).
Samples of sentence reading and conversational speech from 56 IWPDs and
46 HOAs were presented to listeners for ratings of perceived loudness and
intelligibility. Listeners provided ratings of loudness using visual analogue scales
(VAS) and direct magnitude estimation (DME). Acoustic measures of speech level
(e.g. mean intensity), spectral balance (e.g. spectral tilt), and speech level variability
(e.g. standard deviation of intensity) were obtained for comparison with perceived
characteristics. In a spectral manipulation experiment, a gain adjustment altered
the spectral balance of sentence samples while maintaining equal mean intensity.
Listeners provided VAS ratings of perceived loudness of these manipulated samples.
IWPDs were quieter, less intelligible, and had a relatively greater
concentration of low-frequency energy than HOAs. Speech samples with weaker
contributions of mid- (2-5 kHz) and high-frequency (5-8 kHz) energy were
perceived as quieter. Results of the spectral manipulation experiment indicated that
increases in the relative contribution of 2-10 kHz energy were associated with
increases in perceived loudness. The acoustic time-varying loudness model (TVL)
demonstrated stronger associations with perceived loudness and larger differences
between IWPDs and HOAs, and successfully identified differences in loudness in the
spectral manipulation experiment. Loudness ratings provided with VAS and DME
were consistent, both providing excellent reliability.
Findings of this investigation indicate that perceived loudness, acoustic
loudness, and spectral balance are important components of hypophonia
evaluation. Incorporating spectral manipulation in amplification by increasing high frequency
energy may improve efficacy of amplification devices for hypophonia
management.
2. Ongoing work related to the development of a Hypophonia Severity Rating Scale.