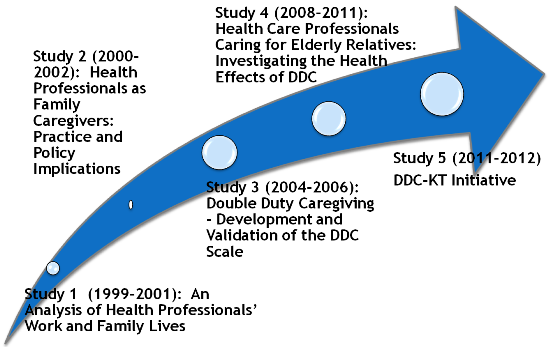
Study 1 (1999-2001)
An Analysis of Health Professionals' Work and
Family Lives
Study 1 Research Summary
Recent changes in patterns of care provision for the elderly have led to an increasing reliance on family care. Although caring has been found to be a central and common feature of the personal and professional lives of many women, this paper discusses the challenges faced by women who provide care in both their work and their family lives ("double-duty caregivers").The author argues that the separation of paid caregiving and unpaid family caregiving in the conceptualizing of elder care is problematic, particularly for health-care professionals. Findings from a qualitative study with registered nurses providing care to elderly relatives revealed that these women are located at the juncture of public and private domains of caregiving, where they must constantly negotiate the boundaries between their professional and personal caregiving roles. The findings highlight the need to explore the interface between women's family and work lives and the need for policies that promote the health of double-duty caregivers.
Funding: Registered Nurses' Association of Ontario (RNAO) ($750.00); SSHRC Internal Grant ($1500); Sigma Theta Tau, Iota Omicron ($650).
Ward-Griffin, C. (2004). Nurses as caregivers of elderly relatives: Negotiating personal and professional boundaries. Canadian Journal of Nursing Research, 36,(1), 92-114.
Recent changes in patterns of care provision for the elderly have led to an increasing reliance on family care. Although caring has been found to be a central and common feature of the personal and professional lives of many women, this paper discusses the challenges faced by women who provide care in both their work and their family lives ("double-duty caregivers").The author argues that the separation of paid caregiving and unpaid family caregiving in the conceptualizing of elder care is problematic, particularly for health-care professionals. Findings from a qualitative study with registered nurses providing care to elderly relatives revealed that these women are located at the juncture of public and private domains of caregiving, where they must constantly negotiate the boundaries between their professional and personal caregiving roles. The
findings highlight the need to explore the interface between women's family and work lives and the need for policies that promote the health of double-duty caregivers.
Ward-Griffin, C., Brown, J., Vandervoort, A., McNair, S., & Dashnay, I. (2005). Double duty caregiving: Women in the health professions. Canadian Journal on Aging, 24,(4), 379-394.
The purpose of this feminist narrative study was to examine the experiences of women in four different health professions (nursing, medicine, physiotherapy, and social work) who provided are to elderly relatives. Although caring is a central and common feature of the personal and professional lives of many women (Baines, Evans, & Neysmith, 1991; Baines, 2004), the separation of professional, paid caregiving from family, unpaid caregiving among health care providers is problematic. Study findings suggest that female health professionals who assume familial responsibilities continually negotiate the boundaries between their professional and personal caring work. Despite the use of a variety of strategies for managing their double-duty caregiving demands, many women experienced a dramatic blurring or erosion of these boundaries, resulting in feelings of isolation, tension, and extreme physical and mental exhaustion. These findings suggest that women, who are double-duty caregivers, especially those with limited time, finances, or other tangible supports, may experience poor health, which warrants further study.
Study 2 (2000-2002)
Health Professionals as Family Caregivers: Practice and Policy Implications
Study 2 Research Summary
The primary aim of this research is to address an issue of critical importance - to identify and evaluate effective strategies for creating supports for family caregivers who are health professionals (nurses, physicians, physiotherapists, social workers). Two main objectives guide the study: 1) identify existing professional polices that help and/or constrain the caregiving efforts of double-duty caregivers (DDC); and 2) create opportunities for inter-professional discipline information exchange and partnership development among four health professional groups (Ontario Colleges and/or Associations of Nursing, Medicine, Physiotherapy, Social Work).
Following the procedures by Krueger (1994) and Brown (1999), four focus groups with health professionals representing the four above disciplines were conducted from a previous study (Ward-Griffin et al., 2001). Focus groups have been used previously to explore health care providers’ experiences in providing care to various populations (Brown, 1999). Each focus group was led by a trained moderator and one of the investigators. The focus group data served as a means to assist with the identification of specific strategies that support DDC efforts at various levels of intervention (individual, family, work, policy). Focus group data also assisted in the development of a key informant interview guide for the current study (see Appendix D).
In-depth semi-structured interviews with key informants of the respective four health professional groups from the Provincial Professional Colleges and/or Associations will be conducted over a two month period of time. Although some of the Colleges require their members to follow certain standards if they care for relatives (see Nursing-College Communique, March 1999), considerable gaps exist between philosophic perspectives and policy implementation. The current study aims to close these gaps by delineating the extent to which various professional practices and polices within each of the Colleges and/or Associations support or hinder individual health professionals in assuming family caregiving responsibilities. Additional demographic information will also be collected (see Appendix E).
A critical focus of this project is to develop and expand partnerships among the four professional colleges and associations with a view to refining/developing new policies aimed at supporting DDC and the elders that they care for. An important avenue for the sharing of information and strategies will be through provincial and local meetings that will bring together professionals, and decision makers representing each of the professional disciplines. The above planned activities meet the objectives of the mandate of the Institute of Gender and Health. Specifically, this proposal focuses on the need for gender specific health policies and strategies for DDC. In addition, it calls for collaborative partnerships among the professional bodies of medicine, nursing, physiotherapy and social work. Any evaluation of gender and health equity as it pertains to the demands of multiple roles must recognize the broader socio-political context of caregiving (Gregor, 1997; Hooyman & Gonyea, 1995; Martin Mathews & Rosenthal, 1993; McKeever, 1994; Pavalko & Woodbury, 2000). This proposal is particularly timely as it responds to the quality of caregivers’ lives and the elders that they care for within a climate of health care restraint. Recognizing the impact of double duty caregiving on women’s (and men’s) health can serve to identify needed policies that will address gender inequities. Indeed, the current proposal will contribute meaningfully to policy by providing evidence concerning the professional practices associated with gender inequities in health among double duty caregivers and the health of Canadian seniors.
References
Brown, J. B. (1999). The use of focus groups in clinical research. In B.F. Carbtree & W. L. Miller (Eds) (2nd ed.) Doing Qualitative Research (pp. 109-124). Thousand Oaks, CA: Sage.
Gregor, F. (1997). From women to women: Nurses, informal caregivers and the gender dimension of health care reform in Canada. Health and Social Care in the Community, 5(1), 30-36.
Krueger, R.A. (1994). Focus Groups: A Practical Guide for Applied Research. Thousand Oaks: Sage
Hooyman, N. & Gonyea, J. (1995). Feminist perspectives on family care: Policies for gender justice. Thousand Oaks: Sage.
Martin Mathews, A. & Rosenthal, C. (1993). Balancing work and family in an aging society: A Canadian experience. In G. Maddox and M. P. Lawton (Eds.), Annual Review of Gerontolgy and Geriatrics 13, 96-119.
McKeever, P.(1994). Between women: Nurses and family caregivers. Canadian Journal of Nursing Research, 26(4), 15-21.
Pavalko, E. & Woodbury, S. (2000). Social roles as process: Caregiving careers and women’s health. Journal of Health and Social Behaviour, 41(March), 91-105.
Ward-Griffin, C. (2000). Women’s personal and professional caregiving: A feminist analysis. The 6th Annual Qualitative Health Research Conference, Banff, Alberta.
Ward-Griffin, C. Brown, J. Vandervoort, A. & McNair,S. (2001).Eldercare in an aging society: Analysis of health professionals’ work and family lives. The 17th World Congress of the International Association of Gerontology, Vancouver, British Columbia
Funding: Canadian Institutes of Health Research (CIHR) Institute of Gender and Health ($8,283).
Ward-Griffin, C. (2008). Health professionals caring for aging relatives: A professional or personal issue? In A. Martin-Matthews, & J. Phillips (Eds.), Ageing and caring at the intersection of work and home life: Blurring the boundaries (pp. 1-20). New York: Taylor & Francis/Psychology Press.
Study 3 (2004-2005)
Double Duty Caregiving: Development and Validation of the DDC Scale
Study 3 Research Summary
Purpose
The purpose of this study was to develop and validate an instrument, the Double Duty Caregiving (DDC) Scale (formerly named the Role Augmentation Scale), which was designed to measure the familial expectations, supports, negotiating strategies and caregiving interface of personal and professional caregiving amongst nurses. Based on a critical feminist perspective (Ungerson, 1990), it is hypothesized that health professionals who report high expectations to provide familial care with limited supports will experience a large degree of caregiving interface, resulting in poorer health outcomes. Specifically, study results identified the: 1) the degree of expectations to provide familial eldercare amongst nurses; 2) the degree of supports amongst nurses who provide familial eldercare; 3) the relationship between expectations to provide familial eldercare and identified supports; 4) the extent of negotiating strategies to help contain expectations and/or expand supports amongst nurses who provide familial eldercare; 5) the caregiving interface amongst nurses who provide familial eldercare; and 6) compare health outcomes of nurses who have varying degrees of expectations, supports and caregiving interface.
Research Methods
Instrument Development: To develop the initial item pool for the DDC Scale, an extensive review of the literature was conducted. In addition, previously collected qualitative data of 38 double-duty caregivers representing four health disciplines (Ward-Griffin et al., 2005) were used to inform the development of the instrument. Consistent with the initial conceptualization of double duty caregiving, items on the DDC Scale were developed to reflect 4 dimensions of double-duty caregiving – expectations to provide familial care, supports, negotiating strategies, and caregiving interface.. Since it is essential that the inductively-derived meaning of double-duty caregiving be preserved in a quantitative instrument (Imle & Atwood, 1988), judgements about clarity, internal consistency and content validity were judged by a panel of four double-duty caregivers. These content experts were asked to rate the relevance of the items on the instrument independently, using a 4-point scale ranging from not relevant to very relevant, thereby facilitating a systematic means of determining revision needs. Raters were also asked whether the conceptual domain of each subscale has been adequately represented by the set of items. Content Validity Indexes (CVI) for each item, subscale and total instrument were calculated, setting the criteria for acceptance at 0.80 (Waltz et al.) Once all items were judged to reflect the overall phenomena of double-duty caregiving, the DDC scale, along with previously tested, well-established measures of role strain (The Women’s Role Strain Inventory, WRSI), caregiver well-being (Tebb Scale); and health and well-being (SF-12), as well as a short demographic questionnaire, were sent to 800 female registered nurses randomly selected from the registry list of the College of Nurses of Ontario (CNO). Following a modified Dillman method, three reminder letters were sent to those who had not returned the completed questionnaires. A total of 384 completed questionnaires were returned. Data from all returned survey packages were edited, coded and entered into SPSS database. Six of these were unusable bringing the final number of questionnaires to 378.
Preliminary Results
Sample: Study respondents (n= 378) ranged in age from 41 to 65 years, with a mean of 51 years. While there was a large range of cultural backgrounds represented, many described themselves as Canadian or Anglo-saxon. Majority of the respondents were married or living common law (74%) who had children living with them (63%). Most held a diploma in nursing (69%), worked full time (97%) in hospital nursing (66%). Fifty-two per cent of the respondents were providing care to one or more elderly relatives (n=198). Most elderly relatives receiving care were parents or parents-in law (89%), who lived less than 10 km from the respondent (49%).
DDC Scale Validation: Currently, a factor analysis of DDC scale (n=190) has been done to help refine the items into subscales. Once item analysis and deletions are completed, Chronbach’s alpha reliability coefficients of at least 0.70, which is adequate for an immature scale (Nunnally & Bernstein, 1984), will be set for the DDC scale. Criterion-related validity of the DDC will also be assessed by correlating the DDC scores with those of the WRSI, The Tebb Scale and the SF-12. To address relationships between
Dissemination of Results: Oral presentations have been delivered/accepted at refereed provincial, national and international conferences:
Ward-Griffin, C. (2005 November). Health professionals caring for elderly relatives: Negotiating the public-private divide. Gerontological Society of America: 2005 Annual Conference . Orlando, Florida.
Ward-Griffin, C. et al. (2006, April). Negotiating personal-professional boundaries: Nurses caring for aging relatives. 25th Annual Conference, Ontario Gerontology Association, Toronto, Ontario.
Ward-Griffin, C. et al. (2006, July).Nurses caring for aging relatives: Blurring the professional-personal boundaries. 17th International Nursing Research Congress, Sigma Theta Tau International Honor Society of Nursing, Montreal, Quebec.
Other Deliverables: A number of undergraduate and graduate students have worked within the project as research assistants/trainees. All of them have learned about the process of mixed methods (e.g. using qualitative data to inform the development of a quantitative instrument), instrument development, and statistical analyses.
Next Steps: We plan to develop and submit a full proposal for a national operating grant in fall of 2006.
References
Imle, M. & Atwood, J. (1988). Retaining qualitiative validity while gaining quantitative reliability and validity: Development of the transition to parenthood Concerns Scale. Advances in Nursing Science, 11(1), 61-75.
Nunnally, J. & Bernstein, I. (1994). Psychometric Theory (3rd edition). New York: McGraw-
Hill.
Ungerson, C. (1990). The language of care: Crossing the boundaries. In C. Ungerson (Ed.), Gender and caring: Work and welfare in Britain and Scandinavia (pp. 8-33). New York: Harvester.
Ward-Griffin, C., Brown, J. B., Vandervoort, A. & McNair, S., Dashnay, I. (2005).
Double-duty caregiving: Women in the health professions. Canadian Journal on Aging, 24 (4) 379-394
Funding: SSHRC (Internal) ($6,920); Canadian Institute of Health Research (CIHR) Institute of Gender and Health ($10,000).
Ward-Griffin, C., Keefe, J., Martin-Matthews, A., Kerr, M., Belle-Brown, J., & Oudshoorn, A. (September 2009). The development and validation of the Double Duty Caregiving Scale (DDCS). Canadian Journal of Nursing Research, 41(3):108-28.
In order to gain an understanding of double duty caregiving (DDC), defined here as the provision of care to elderly relatives by practising health professionals, a DDC scale has been developed. This study tests the psychometric properties of the scale. Survey data were collected from a random sample of 187 female registered nurses who were employed and also provided care to elderly relatives. Nine factors contributing to DDC emerged from exploratory factor analysis. The DDC subscales were moderately correlated with the standardized health measures included in the study.The caregiving interface (degree of blurring between the professional and personal caregiving domains) was significantly negatively correlated with well-being and mental health.This result extends our understanding of the supports needed by those providing DDC.
Study 4 (2009-2011)
Health Professional Caring for Elderly Relatives: Investigating the Health Effects of Double Duty Caregiving
Study 4 Research Summary
Purpose
The purpose of the study was to test the model of double duty caregiving (DDC) and to determine if and to what degree DDC impacts the health of professional caregivers.
Study Goals
By using both quantitative and qualitative approaches, we made visible what has been "invisible"- caregiving at the juncture of professional and personal caregiving domains. These study findings informed health professional policies (e.g. Best Practice Guidelines (BPGs)) related to the blurring of professional and personal boundaries among male and female RNs in Canada. In keeping with the theoretical framework of the study and with past practices of the investigative team, researchers worked with health providers, professional organizations and policy makers to promote the uptake of the study findings, as well as worked to inform the refinement and development of policies. Ultimately, study findings promote an evidenced-base partnership approach that will address the potential health effects of double duty caregiving.
Phase I – Quantitative (survey)
We used a cross-sectional survey design to validate the measurement scales employed in the proposed DDC model, and to test the following hypotheses:
- Expectations have a positive effect on Caregiving Interface;
- Supports have a negative effect on Caregiving Interface;
- Making Connections and Setting Limits have a negative effect on Caregiving Interface;
- Caregiving Interface has a negative effect on Health.
3700 male and female RNs in British Columbia, Ontario, and Nova Scotia were invited to complete a mailed or online survey, with the aim to test the DDC Measurement Model.
Structural Equation Modeling techniques were employed to conduct these tests. Furthermore, comparison of DDC scores by gender with respect to health status, well-being, and burnout were also conducted.
Phase II – Qualitative (interview)
A grounded theory approach was used to further explore the three proposed prototypes of DDC (making it work, working to manage and living on the edge). Using a purposive sample of DDCs selected from Phase I who fall within these prototypes, we explored how male and female DDCs mediate the caregiving interface and resulting health effects. Through the use of repeat interviews (Time 1 and Time 2), theoretical sampling helped to enhance our understanding of the possible caregiver oscillation within these three DDC prototypes found in our initial qualitative work of DDC. Participants were also asked to describe the impact of policies (or lack of) on their health as DDCs and to recommend any changes that could address their issues/concerns.
Concurrent with data collection, data were analyzed using the constant comparison methods of constructivist grounded theory, modifying the emerging theory such that it fits both the new data and the relevant constructs within the prototypes of DDC.
Funding: Canadian Institutes of Health Research ($200,000)
Ward-Griffin, C., St-Amant, O., & Brown, J. (2011). Compassion fatigue within double duty caregiving: Nurse-daughters caring for elderly parents. Online Journal of Issues in Nursing (OJIN).
This article examines compassion fatigue within double duty caregiving, defined here as the provision of care to elderly relatives by practicing nurses. Using qualitative data from our two studies of Canadian double duty caregivers, we identified and interviewed 20 female registered nurses whom we described as "living on the edge." The themes of context, characteristics, and consequences emerged from the findings. In this article, we argue that being both a nurse and a daughter leads to the blurring of boundaries between professional and personal care work, which ultimately predisposed these caregivers to compassion fatigue. We found that the context of double duty caregiving, specifically the lack of personal and professional resources along with increasing familial care expectations, shaped the development of compassion fatigue. Nurse-daughters caring for elderly parents under intense and prolonged conditions exhibited certain characteristics, such as being preoccupied and absorbed with their parents' health needs. The continual negotiation between professional and personal care work, and subsequent erosion of those boundaries, led to adverse health consequences experienced by the nurse-daughters. The study findings point to the need to move beyond the individualistic conceptualization and medical treatment of compassion fatigue to one that recognizes the inherent socio-economic and political contextual factors associated with compassion fatigue. Advocating for practice and policy changes at the societal level is needed to decrease compassion fatigue amongst double duty caregivers.
Research Summary (contact Principal Investigator for copyright)
|
